OPHTHALOMOLOGY
Vision
The JR. Borja General Hospital- Ophthalmology Department, recognized by patients and staff for excellence and compassion in service and care.
Mission
We will provide quality eye care that inspire patient first, integrated, accessible, cost effective, and appropriate to the community's needs.
To our patients, we commit to improve quality of life by providing exceptional eye care, through a safe and caring environment.
To community, we pledge to support the neighboring community by participating in any Medical Mission related activity and other initiatives that will help improve and prevent vision impairment within our region and country.
Our Core Values
INTEGRITY – We are committed to the highest ethical standards, uprightness and honesty. We operate in adherence to professional conduct to ensure transparency and fairness within the workplace.
COMPASSION - We treat everyone with kindness, respect and dignity. We will empathize with and demonstrate sensitivity to patients and their families and help them to the best of their ability.
COMMITMENT- The Ophthalmology Department shares the mission and vision of the hospital and will do our part to achieve them.
PROFESSIONALISM- We uphold the rules and regulation of our profession to ensure, the standard of service and quality of medical care.
OPENNESS- We are open to ideas, suggestions and feedback so as to continuously improve and innovate our eye care services.
Our Objectives
- To establish a complete, competitive and modern eye care facility that provides affordable, equitable and accessible eye care.
- To establish a clinic that can cater to most, if not all ophthalmic needs. This includes engaging in sustainable eye health education, maintaining and broadening our reach and access to our partner communities; and complying with social responsibilities.
- To develop a team of well-trained and dedicated allied health personnel.
- To create a happy, healthy, harmonious and safe workplace.
Organizational Structure
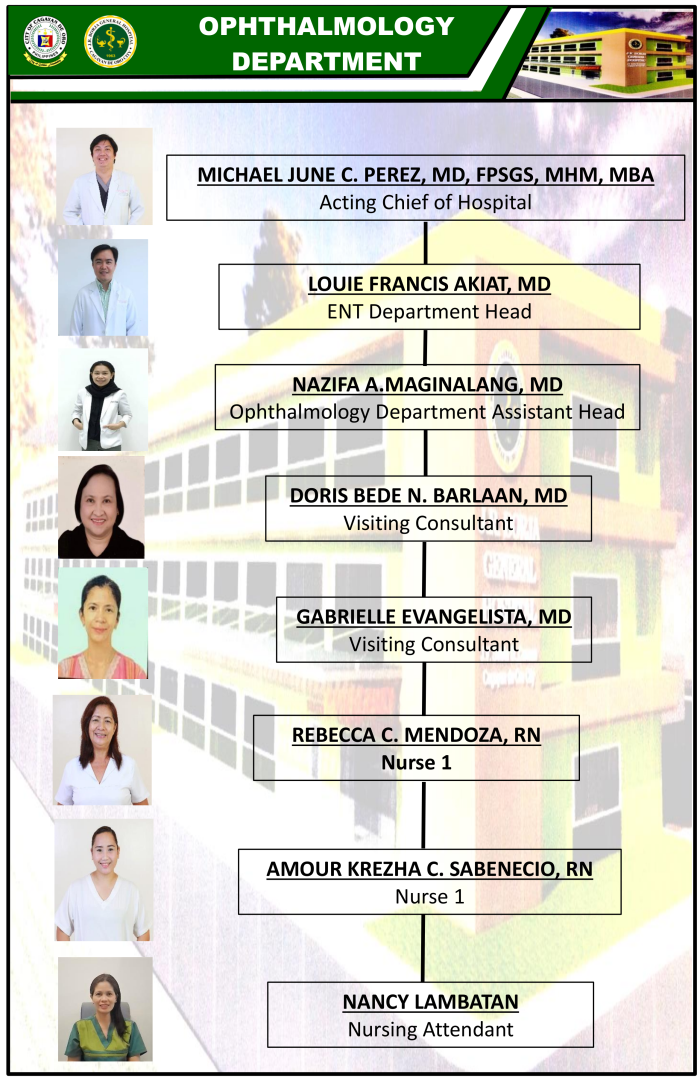
Organizational Chart
The Department of Ophthalmology is under the Surgical Division. It shall be headed by a Department Chairperson and Vice-Chairperson. Other positions shall be created upon the discretion of the Department Chair and upon approval of the Medical Division Chief and the Chief of Hospital.
All programs, units and/or sections handled by the Department shall have Heads who shall directly report to the Department Chair.
Physical Set-Up
The Department of Ophthalmology is divided into 4 distinct areas:
The Eye Center
It is situated at the 2nd floor of the OPD Building adjacent to the Telemed Office. It houses the following:
1) General Ophthalmology/Subspecialty Clinic
2) Minor Operating Room
3) Conference Room
4) Eye Instrument Center
5) Reception and Seating Area
The Ophthalmology ER
It is located at the Emergency Room Complex of the hospital. It has a small corner with a slit lamp, visual acuity chart and minor surgical bay.
It serves an average of 50 trauma and non-trauma consultations and referrals per month.
The Ophthalmology Ward
The department’s ward is located at the 2nd floor of the main building. There is only one ward for both male and female with 5 beds each for service cases.
The Ophthalmology OR
The Ophthalmology Operating room is located at the OR Complex in the 2nd floor of the main hospital. It is divided into 2 sections. One bed caters clean cases (cataract and glaucoma) and the other bed is for major ophthalmic procedures (Orbit & Oculo-plasty, Pediatric Ophthalmology, ED/Cornea) and potentially infected cases including emergency trauma cases requiring general anesthesia.
The department handles more than 30 surgical cases every month.
Programs and Committees
Ophthalmologist may be assigned to play roles in the following Hospital Programs and Committees:
- Pharmaceutical and Therapeutics Committee
- Telehealth Committee
- Patient Safety Committee
- Forms Committee
- Occupational Safety and Health
- Antimicrobial Stewardship Program
- Infection Prevention and Control
- Quality Management Systems
Standard Operating Procedures
THE OPHTHALMOLOGY EMERGENCY ROOM AND ER PATIENT CARE
- During office hours, an ER Ophthalmologist-in-charge (OIC) is assigned to attend to and take responsibility for patients referred to the Ophthalmology ER.
- The OIC is expected to promptly attend to all emergency cases and referrals within 30 minutes from the time of referral. The ER OIC shall render appropriate medical care to all Ophthalmology ER patients and referrals.
- The OIC shall write the complete findings made during examination, the assessments and the plans for diagnosis and treatment in the ER Form. The ER Form should be signed and his name stamped below the signature.
- The OIC shall personally make all the requests for laboratory and ancillary procedures necessary for the diagnosis and treatment of the patient’s conditions.
- Informed consents must be secured for all surgical procedures necessary for diagnosis and treatment by the OIC performing such (including foreign body removal, irrigation, conjunctival membrane removal).
- In case of the need to refer to another specialty in the ER, the OIC must make the necessary arrangements and facilitate the referral.
- All initial ER consults that are clear-cut sub-specialty cases that can be followed up on an out-patient-basis must be referred or transferred after giving appropriate ER treatment to the sub-specialty discipline concerned at the nearest sub-specialty clinic schedule.
- All ER consults, requiring admission shall be admitted under the service of the OIC. Patients who are clear-cut sub-specialty cases are expected to be referred or transferred to the sub-specialty discipline concerned at the soonest possible time even on weekends and holidays.
- The ER OIC should personally prescribe medications in generic notation, give advice and provide home instructions.
- The ER OIC shall provide a follow-up appointment slip. The notation should be signed and his name stamped below the signature.
- If a patient needs to be admitted, the ER OIC write the admitting notes and history, and make the necessary arrangements with the Admitting Office, the Ward and the OR (if needed).
- The ER OIC shall make sure that the Trauma Registry Forms are properly accomplished and that all cases are completely logged.
- The ER OIC should see to it that all instruments are clean and in order.
THE WARD AND IN-PATIENT CARE
- OIC shall render appropriate medical care to all patients admitted under his care, and to all other patients he is called to attend to during his/her tour of duty in the hospital. There shall be no delay in performing the physical examination of a patient. In case of a pending surgical procedure scheduled after the duty, it remains the responsibility of the service-in-charge to perform the procedure.
- The OIC shall be responsible for accomplishing the admitting history of elective cases and shall perform the necessary evaluation within the first 24 hours of admission
- The OIC shall promptly respond when called upon. He shall note the date and time the call was received. He shall write his findings, the date and the time they were noted and the measures taken in the Staff/Progress Notes sheet of the chart, not in the Physicians Order Sheet.
- All orders must be legibly written in the physicians’ order sheet by the OIC. When writing orders, they should indicate the date and time the order was made. His signature shall be affixed above the stamp bearing his name.
- The OIC shall make daily rounds and do progress notes on their in-patients from 7:00AM - 8:00AM on weekdays. The OIC shall also make daily rounds prior to leaving the hospital at the end of the work day. On weekends and holidays, the OIC should accomplish the above by 12 noon.
- The OIC shall ensure that all doctors’ orders are carried out. In case there is a delay or the order was not carried out, the reasons for these should be written in the staff/progress notes sheet of the patient chart. The ROD shall ensure that
- all orders prescribed by the non-duty service/s at the end of the work day are carried out
- The OIC of in-patients should be done at the Eye Center. He shall additionally visit patients who are in critical condition as often as the situation demands
- The OIC shall facilitate referrals of patients needing further evaluation to other departments during office hours. The COD shall assume this task after office hours.
- The OIC is responsible for accomplishing and signing the discharge summaries of patients before they are sent home. For service patients, a photocopy of the discharge summary and progress notes should be inserted in the patient’s Chart.
- Before discharging a patient, the OIC should provide home instructions and prescription for medications, issue a follow-up appointment or write the date of follow-up in the Eye Card (if available). His signature shall be affixed above the stamp bearing his name.
THE OPERATING ROOM AND SURGICAL PROCEDURES
- The OIC shall be responsible for scheduling elective surgical procedures at the Main Hospital OR and Minor Operating Rooms and shall hold pre-operative meetings with the Service Teams and Ophthalmology OR Nurses with regards to major surgery.
- The Service Teams shall be responsible for explaining the procedure to patients, securing consent forms, prescribing surgical needs, borrowing surgical equipment and proper scheduling of the surgery.
- OIC assigned at the operating room are expected to be there no less than 30 minutes prior to the scheduled OR procedure. Notwithstanding the duties of the OR nurses, the OIC are ultimately responsible for calling the patient for surgery to the OR one (1) hour prior to the scheduled surgery under general anesthesia. This is to allow for the administration of anesthesia pre-medication/s, transport of patients from ward to OR and timely pre-operative patient preparation.
- Patients’ Safety Checklist and proper Time-Outs shall be observed and adhered to at all times prior to any surgery.
- For patients under general anesthesia, the OIC should be present prior to induction and during emergence from anesthesia.
- The OIC shall be responsible for accomplishing the operative technique, issuing post-op orders and prescriptions, as well as, home instructions for outpatient procedures.
- It is the duty of the surgeon / service team to inform the patient’s relatives of the outcome and/or prognosis of the surgical intervention as they become necessary.